
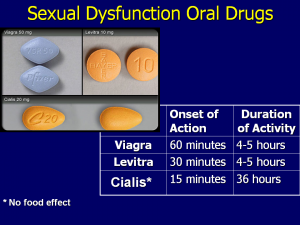
It’s been 18 years since the FDA approved sildenafil to treat men suffering from erectile dysfunction (ED). Under the well-known brand name Viagra, this “little blue pill” has grown to hold almost half of sexual dysfunction market share.
But, sildenafil wasn’t originally intended to help men with ED. Many have forgotten that before it was associated with a re-invigorated love life, sildenafil was a life-saving drug for people experiencing cardiovascular problems.

cGMP and PDE5 inhibitors
The groundbreaking discovery of nitric oxide (NO) in 1986 was the launch point for a novel innovation in drug discoveries. NO is a potent vasodilator that relaxes blood vessels and encourages blood flow (1).
Researchers found that NO is a critical mediator for several physiological systems that regulate blood pressure, prevent the development of atherosclerosis, and maintain penis erection. Because NO has such an incredible vasodilatory effect, it’s considered one of the most essential modulators of blood pressure.
NO accomplishes this by the formation of a substance called cyclic guanosine monophosphate (cGMP). The enzyme responsible for stopping cGMP is called phosphodiesterase enzyme 5 (PDE-5). This enzyme is always observed at high levels in patients experiencing conditions like heart failure or ventricular hypertrophy.
The discovery of PDE-5 inhibitors like sildenafil opened up a whole new approach to dealing with circulatory problems. Sildenafil provided a effective way to both restore and maintain healthy circulation, especially in people suffering from cardiovascular disease (2).
Pfizer develops a heart drug with an unusual side-effect
By the early 90s drug giant Pfizer had completed several trials of sildenafil citrate as a treatment for angina with little evidence that it was a sufficiently effective option. But, included in data collected from volunteers was anecdotal evidence that they were experiencing increased erections for several days after taking the drug.
Pfizer decided to go ahead with pilot studies with patients experiencing erectile dysfunction. In 1996 Pfizer acquired a US patent for sildenafil citrate and by March 1998 it was FDA approved to treat ED and pharmacists began dispensing it under the brand name Viagra.
Erectile dysfunction
ED is a common sexual disorder affecting millions of men worldwide. Over half the population over 40 years old experience some degree of ED. Some of the risk factors for ED are:
- Sedentary lifestyle
- Injuries
- Alcohol consumption
- Excessive stress
- Smoking
Among the most common treatment options that are available, PDE-5 inhibitors have become the most preferred by physicians for increasing blood flow and relaxing muscles for improved erections (3).
There were worries about safety
In 2000, research was presented by Dr. Sanjay Kaul at the 49th annual Scientific Session of the American College of Cardiology that suggested that there were 522 Viagra-related deaths in the first year the drug entered the market. While not explicitly blaming sildenafil the doctor was quoted by WebMd as saying, “Data appears to suggest that there’s a relatively high number of deaths and adverse cardiovascular events associated with the use of Viagra.” He also clarified that he was not implying any cause-and-effect relationship.
More recent studies have firmly established that PDE-5 inhibitors are safe, well-tolerated by most people, and have generally mild side-effects (4, 5, 6).
According to research PDE-5 inhibitors can treat more than ED
The clinical use of PDE-5 inhibitors has now come full circle. Although the original trials failed to demonstrate efficacy for the treatment of angina, hypertension, and other cardiovascular conditions, more recent studies have concluded otherwise. Due to the multiple cellular processes involving PDEs, inhibitors have found new applications in the treatment of some medical conditions (7).
Sildenafil for pulmonary hypertension
Sildenafil will help cases of pulmonary arterial hypertension (8); a lung disorder resulting from the narrowing of arteries (pulmonary arteries) that carry blood from the heart to the lungs. This narrowing causes abnormally high blood pressure in the pulmonary arteries that strains the right ventricle of the heart and causes it to expand. If it continues long enough the right ventricle will lose the ability to pump sufficient blood to the lungs, possibly leading to heart failure. Sildenafil is marketed under the brand name Revatio to treat pulmonary hypertension.
Benefits extend to diabetics
Sildenafil has been shown to reduce diabetes-induced oxidative stress and even improve insulin sensitivity to prevent type 2 diabetes (9). According to research in the Journal of Clinical Endocrinology and Metabolism, sildenafil can not only treat ED but will prevent type 2 diabetes in patients experiencing pre-diabetes, while it reduces the risk of kidney and heart disease.
It raises serum testosterone levels
20 patients at an average age of 55 years were given the PDE-5 inhibitor Tadalafil over a 12-month study period. Researchers observed sustained improvement in the men’s sexual function after one year. Tadalafil administration was associated with increased testosterone and reduced estrogen levels. The theory is that chronic exposure to tadalafil might improve the hormonal profile that regulates erectile function (10).
Can effectively treat prostate enlargement
Benign prostatic hyperplasia or BPH (prostate enlargement) and ED are not only linked by similar risk factors like age and cardiovascular disease but also at a molecular level. According to studies, PDE-5 inhibitors are a practical treatment option to relieve moderate to severe urinary symptoms of BPH (11).
PDE-5 inhibitors and premature ejaculation
Premature ejaculation (PE), while not a physically harmful condition, causes psychological distress in men who suffer it. A recent study (12) looked at whether sildenafil could increase the time to ejaculation and reduce the time needed to become erect again. The study concluded that sildenafil used alone wasn’t better than a placebo or combination treatment to treat PD.
The importance of an erectile dysfunction panel
An ED panel is a laboratory investigation looking at the possible hormonal causes of a patient’s ED. While an ED panel isn’t necessary for everyone experiencing erectile problems, it’s still a good idea.
An ED panel will determine your levels of:
- Prolactin
- Total and Free Testosterone levels
- Sensitive Estradiol
- DHT
- TSH
- Free T3
- Free T4
An imbalance in any of these hormones could cause low libido/ ED. Before you consider medication to treat your ED, you should first consider investigating if there is another medical issue that may need to be addressed.
References
1) Musicki B, Champion HC, Becker RE, Liu T, Kramer MF, Burnett AL. Erection capability is potentiated by long- term sildenafil treatment: role of blood flow-induced endothelial nitric-oxide synthase phosphorylation. Mol Pharmacol.(2005)
2) Chester AH, O’Neil GS, Moncada S, Tadjkarimi S, Yacoub MH. Low basal and stimulated release of nitric oxide in atherosclerotic epicardial coronary arteries. Lancet. (1990)
3) Olsson AM, Speakman MJ, Dinsmore WW, et al. Silde- nafil citrate (Viagra) is effective and well tolerated for treating erectile dysfunction of psychogenic or mixed aetiology. International Journal of Clinical Practice. (2000)
4) Steers W, Guay AT, Leriche A, et al. Assessment of the efficacy and safety of Viagra (sildenafil citrate) in men with erectile dysfunction during long-term treatment. Int J Impot Res. (2001)
5) Porst H, Giuliano F, Glina S, et al. Evaluation of the efficacy and safety of once-a-day dosing of tadalafil 5 mg and 10 mg in the treatment of erectile dysfunction: results of a multicenter, randomized, double-blind, pla- cebo controlled trial. Eur Urol. (2006)
6) Brock G, Nehra A, Lipshultz LI, et al. Safety and efficacy of vardenafil for the treatment of erectile dysfunction after radical retropubic prostatectomy. J Urol. (2003)
7) Kukreja RC. Cardiovascular protection with sildenafil following chronic inhibition of nitric oxide synthase. Br J Pharmacol. (2007)
8) Galie N, Ghofrani HA, Torbicki A, et al. Sildenafil citrate therapy for pulmonary arterial hypertension. N Engl J Med.(2005).
9) Milani E, Nikfar S, Khorasani R, Zamani MJ, Abdollahi M.Reduction of diabetes-induced oxidative stress by phos- phodiesterase inhibitors in rats. Comp Biochem Physiol C Toxicol Pharmacol. (2005)
10) Greco EA, Pili M, Bruzziches R, Corona G, Spera A, Aversa A. Testosterone:estradiol ratio changes associated with long-term tadalafil administration: a pilot study. J Sex Med. (2006)
11) Uckert S, Oelke M, Stief CG, Andersson KE, Jonas U, Hedlund P. Immunohistochemical distribution of cAMP- and cGMP-phosphodiesterase (PDE) isoenzymes in the human prostate. Eur Urol. (2006)
12) Atan A, Basar MM, Tuncel A, Ferhat M, Agras K, Tekdo- gan U. Comparison of efficacy of sildenafil-only, silde- nafil plus topical EMLA cream, and topical EMLA-cream- only in treatment of premature ejaculation. Urology. (2006)












")

{kind=link}